
I have received A LOT of questions lately about corridor doors in health care occupancies. As many of you know, I like to find concrete answers but it isn’t always possible, and sometimes I uncover an area that requires a code change to clarify what is required. Because the code development cycle is typically 3 years, it can take a while to make a change, and meanwhile the answer will be up to the interpretation of the AHJ.

Rescue hardware allows an inswinging door to become outswinging, by incorporating center pivots, a double-lipped strike, an emergency stop and a cased opening frame.
A recent question was with regard to rescue hardware on corridor smoke partition doors in a hospital, nursing home, or behavioral health facility. If you’re not familiar with rescue hardware, it is a combination of products which allow an inswinging door to become outswinging if someone falls inside the room or purposely tries to barricade the door. The system typically includes center pivots or a special double-swing hinge, a double-lipped strike which protects the frame, and an emergency stop that can be pushed into the jamb to allow the door to swing out (LCN has a special template for a closer too). Because the door has to swing in both directions, the frame is a cased opening frame, which has no stop at the head or jambs.
Current codes do not require fire door assemblies on many of the doors in corridor smoke partitions, such as patient room doors, bathrooms, or tub/shower rooms. Some corridor doors will require a fire rating, like doors to exit enclosures and large storage, waste, or linen collection rooms, but the doors that do not require rated opening protectives are only required to provide an effective barrier to limit the passage of smoke. The question is – what constitutes an effective barrier? Without the frame stop there is nothing to limit the passage of smoke through the clearance around the door unless gasketing is installed, and is that gasketing enough?
For smoke doors in some other locations, air infiltration limits are established and openings tested to UL 1784 – Air Leakage Tests of Door Assemblies. However, UL 1784 is not referenced in the section of the International Building Code that describes the requirements for corridor doors in hospitals and nursing homes (407.3.1 in the 2009, 12, and 15 editions).
Adding to the confusion, the IBC Commentary uses the doors described in section 407.3.1 as an example of doors that need to be tested per UL 1784, even though there is nothing in section 407.3.1 stating this requirement. If the Commentary is correct, it would require smoke gasketing on every smoke partition corridor door, which is not typical. I asked the ICC for a staff opinion on this, and received confirmation that UL 1784 testing is not required for non-fire-rated corridor doors, but that the door must provide an effective barrier to limit the passage of smoke. But what constitutes an effective barrier?
NFPA 101 – The Life Safety Code (2012 edition) is a little more clear on this topic, at least when it comes to toilet, tub, and shower rooms. For new health care occupancies, section 18.3.6.3.1 requires corridor doors to be constructed to resist the passage of smoke, but exempts doors to toilet rooms (and similar types of rooms that do not contain flammable or combustible material) from the smoke resistance requirement. So in my opinion, NFPA 101 would allow rescue hardware on toilet rooms. But what about patient rooms? Rescue hardware is becoming much more common on behavioral health facilities, to prevent patients from barricading the door. NFPA 101’s Annex A states, “Gasketing of doors should not be necessary to achieve resistance to the passage of smoke if the door is relatively tight-fitting.” Would a door with rescue hardware be considered relatively tight-fitting? How about if it had a privacy gasket mortised into the edge?
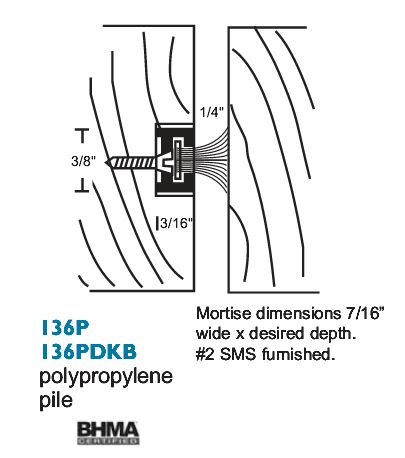
National Guard Products mortised gasketing is often used for doors with rescue hardware to provide privacy.
I asked the Joint Commission for their opinion, and the response I received confirmed that 1/8-inch clearance at the head and jambs is acceptable for a smoke resistive corridor door per the Joint Commission standards (1-inch maximum at the bottom of the door). The response also stated that “Closing the gap with gasketing material would be prudent.”
Looking at it from a common sense standpoint, I don’t know if gasketing for toilet rooms is really necessary for smoke infiltration (although it is recommended at the vertical edges for privacy). If there was a fire, what are the chances that a) the fire would be in the bathroom and the door would be needed to prevent smoke from entering the corridor, or b) the fire would be elsewhere and someone would be sheltering in the bathroom and need protection from smoke? But for patient room doors with rescue hardware, I think gasketing at the head and jambs makes sense, although behavioral health safety concerns need to be considered when products are selected. Until the code is clarified, that’s all I’ve got, and ultimately it is up to the AHJ to decide.
What do you think?
Thank you to Paul Goldense of Goldense Building Products for letting me tag along on a visit to a behavioral health facility last week!
Gasketing Graphic: National Guard Products
You need to login or register to bookmark/favorite this content.




CMS issued an interpretation on this earlier in the year. I was surprised at the generosity of the tolerances. Perhaps one of your readers has the S&C number for a reference.
Keep in mind that the pivots are ‘center hung’–which means they need a radiused edge on the heel of the door. I don’t believe that Ives–or others–have those pivots UL listed.
Hi Terry –
The doors in question do not require a UL listing. They just have to be an effective barrier to limit the transfer of smoke.
– Lori
The effective smoke/draft barrier according to UL 1784 is limited to 3 cu ft per minute per sq foot of door at 0.10 inch water gage for both ambient and elevated temp tests. If UL 1784 does not apply then Lori is correct in asking what does qualify as an effective smoke and draft barrier.
Good article! Unfortunately the IBC doesn’t have the exceptions for certain rooms for limiting the transfer of smoke and the requirement of positive latching in Section 407.3 that NFPA has in Section 18.3.6.2.1 & 18.3.6.3.6. Therefore, any use of the NFPA exceptions would have to be approved by the local building authority. You would think they would compare the two codes when writing a new code for some consistency. Just saying.
Hi Mark –
I know the requirements aren’t consistent between codes, but I like to include both especially on these grey areas, to give us some insight into the possible intent and also to identify potential code changes that need to be proposed.
– Lori
Lori: If CMS/JCAHO adopt NFPA 101 – 2012 as it looks like they will sometime in 2015 then won’t the inspection provision for ‘Smoke Doors’ come into play? 101 – 2012 7.2.1.15.2 (basically inspected per NFPA 105 – 2010). If that is the case, and you reference 105-2010 4.3.1, it says that the “Smoke door assemblies shall have an air leakage rating not greater than …..in accordance with ANSI/UL 1784…”. How does this 105 citation come into play for the types of doors referenced in you article above?
Thanks again for another great learning opportunity. You do a great service to the door industry. And I’m not shy about telling your supervisors the same.
Regards, Jerry
Thanks Jerry! It’s always nice for my supervisors to hear the kudos for iDH. 🙂
The problem with “smoke doors” is that the official definition of a smoke door is a bit blurry. There are different doors that you or I might consider smoke doors, but only a few references in NFPA 101 to NFPA 105 that would make it official.
If you look at the section below from the 2012 edition of 101, it clearly says that certain smoke doors must be inspected, but technically it only applies to door assemblies that are required to be smoke-leakage rated, and patient room doors are not required to be smoke-leakage rated. There are other sections that specifically reference 8.2.2.4, like 8.5.4.2 which deals with smoke barrier doors.
8.2.2.4 Where door assemblies are required elsewhere in this Code to be smoke leakage–rated in accordance with 8.2.2.4, door assemblies shall comply with all of the following:
(1) They shall be tested in accordance with ANSI/UL 1784, Standard for Air Leakage Tests for Door Assemblies.
(2) The maximum air leakage rate of the door assembly shall be 3.0 ft 3/min/ft 2 (0.9 m3/min/m2) of door opening at 0.10 in. water column (25 N/m2) for both the ambient and elevated temperature tests.
(3) Door assemblies shall be installed in accordance with NFPA 105, Standard for Smoke Door Assemblies and Other Opening Protectives.
(4) Door assemblies shall be inspected in accordance with 7.2.1.15.
No nut-job has ever unfurled a full roll of TP and lit it on fire??
I don’t know what the accessibility to lighters/matches is…I guess it’s a possibility.
What about when local AHJ requires the patient rooms be a smoke partition? In Seattle patient rooms are required to be a smoke partition and limit the passage of smoke, if UL1784 isn’t required how are you to know it limits the passage of smoke if a non-UL listed system is used?