

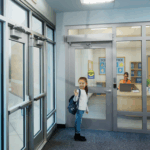
Today’s WWYD question is a tough one, and I’m hoping someone has an idea. The hospital is in Qatar, and the patient room doors are currently equipped with long pulls on both sides, and a deadbolt. The facility is required to provide latching hardware on these doors. The lock must be lockable from the outside and must provide free egress from the inside, but it must not be lockable without a key.
WWYD?




You need to login or register to bookmark/favorite this content.



Interesting
1. Lockable from the outside
2. But still openable from the inside?
3. Or lockable at times and person inside cannot open the door?
4. Do it electronically, some what like a hotel room door?? Card to get in?
Hi Charles –
When it’s lockable from the outside, people on the inside still need to be able to get out. The tough part is providing latching hardware that doesn’t conflict with the pulls. I think the pulls may have to go.
– Lori
Seems like at least on the patient side they would need to be removed, and more than likely on the corridor side also, so staff can get in easily.
Even if you move them, people will still grab them expecting the door to open.
I think the pulls have to go, and put a hospital latch on. If they are in love with the pulls, then put the hospital latch on and put a pull on the top and bottom below the latch.
Is there room for knob trim? If so, then changing out the mortise lock case for an acceptable function (maybe a latch hold-back) may allow you to keep the vertical pulls.
I agree the pulls have to go. But the mortise lock may also be in the way, depending on what height you install the classroom function lever.
I agree Lori, no way to do it properly with the pulls on there. Hopefully the deadbolt is at a height that is acceptable for lever mortise locks, they look a bit high.
I am in agreement that the pulls are a problem. I would try to replace the mortise deadbolt with a latching function with deadbolt that worked on the restroom deadbolt concept. Can only unlock from the inside but not lock. Or a function where the inside lever retracts the deadbolt and there is no inside deadbolt actuation at all. Then a key would be required on the outside to lock the door. Am I thinking Schlage L9460?
Any way to get the pull to activate the latch. Something like the CRL systems for glass doors. Sorry I only did this once and that was nearly a decade ago so I’m not up on their current stuff.
Doors to patient sleeping rooms to an Exit Access Corridor are not permitted to be locked unless :
1) The key-locking device does not restrict egress from the room to the corridor. (The current keyed lock on the patient room side is not compliant),
2) Locks complying with the door-locking arrangements based on the clinical need (e.g. psychiatric rooms) of the patient (see 18.2.2.5 of the 2012 LSC).
The positive latching requirement for corridor doors are per 18.3.6.3.5 (2102 LSC). This would have to be accomplished with a latching device that only requires (1) operation. The keyed lock + the unlatching device would total (2) operations. Roller latches are prohibited unless the door-in-question was serving an “acute psychiatric setting where patient special clinical needs require specialized protection measures” (18.3.6.3.9.2 2012 LSC).
I am not sure of the situation, but if the room needs to be locked by key only from the outside with free egress from inside, would it be to keep people out of an unoccupied room? seen rooms in psych wards that must be opened with key and patients locked in. In this instance however, would a hospital latch and a classroom deadbolt above the hospital latch. Remove existing pulls.
The existing lock is European – appears to be a profile cylinder, also narrower lock case than ANSI standard.
They make a dead bolt with key on the outside
And lever on the inside?
If so could the lever be installed vertically ??
I believe the existing Format deadbolt could likely be swapped out for a Format “narrow style sashlock” which could have levers on both sides and a key x thumbturn euro profile cylinder. Made in 25, 30, 35 and 40mm backsets, see link. Shorten the pulls so that they do not interfere with the levers.
http://www.jgf.co.uk/catalogue.aspx?CategoryRef=3
Peter – thumb turn inside is not a single motion free egress per NFPA 101
The hardware I see has been furnished as per BS/EN standards. The fire rating for doors differs as positive latching is not required for fire rated doors as per BS/EN standards. Now for the patient safety, they should remove the double profile cylinder and replace with a classroom(with thumb-turn) profile cylinder where the door cannot be locked from inside but can be opened from inside if locked.
Door pulls and deadbolt needs to go. There is a reason why Allegion, ASSA, and all the other manufacturers make Hospital latching and locking Hardware.
Pulls have to go. Add Glynn Johnson HL-6-9070 classroom function. You can still use the dead bolt function to lock an empty room, if someone inside when locked the inside thumb turn can only retract the bolt.
Electric Strike and interior sensor to trigger the strike for egress and change the body to a latching deadbolt.
Is it a safe cell for mental health patients maybe? That would be a viable explanation.
This is a typical European hardware and these lock bodies are narrower than ANSI. It would be a difficult retrofit operation if they have to change this to ANSI. My suggestion is to remove the Pulls both sides, and go for Escape locks from European hardware ( from the same manufacturer so that lock case would be modular so no need for much chipping from the door). Typically Escape lock ( Allegion Briton 5660 ) should do the trick. Lever both sides, single cylinder outside. Free egress from inside by operating the lever all the time, From outside you can lock with key. Lock is with split follower. https://www.allegion.co.uk/content/dam/allegionuk/Downloads/Inspec%20datasheets/DS072_Briton5600Series_Locks.pdf