
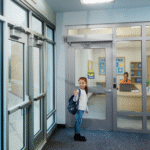
Last week I saw the video below, along with a story in The Blaze. It’s about a father who took his newborn out of a maternity ward in a shopping bag. The baby was born with drugs in her system, and the parents wanted to spend some time with her before she was removed from their care. The father attempted to go through two different doors equipped with delayed egress mag-locks, and both times the alarms were silenced by staff members. When he tried one of the doors again, it allowed him to exit with the baby.
(Scroll down to read about a pertinent code change.)
A video should appear below. If it does not, you can access it here.
FOX 10 News | fox10phoenix.com
There was an important change to the 2015 International Building Code (IBC) that could help to prevent this from happening in the future. Many maternity wards have infant abduction systems that use a sensor to activate a delayed egress lock when a baby is taken near the exit. But for some facilities, delayed egress locks may not be enough.
In the 2009 edition of the IBC and NFPA 101 – The Life Safety Code, code requirements were added that addressed the use of controlled egress locks in health care facilities. In certain areas of hospitals, nursing homes, and other treatment facilities, locks may be installed which prevent egress under normal circumstances. The locks must allow egress during an emergency – either automatically or with staff assistance, depending on the occupancy.
I wrote an article for Locksmith Ledger which addressed the requirements in the 2012 editions of the IBC and NFPA 101, but the 2015 edition of the IBC includes some important changes to this section (1010.1.9.6). Previously called “special egress locks,” the IBC now uses the term “controlled egress.” In the 2009 and 2012 editions of the IBC, this section applied to I-2 use groups, but now applies to I-1 and I-2 facilities. Some of the terminology has changed slightly, clarifying the types of locks that can be used (electromechanical or electromagnetic) and where previous editions allowed these locks to be used “where the clinical needs of persons receiving care require such locking,” the 2015 edition references a need for containment. I expect that the 2015 IBC Commentary, available soon, will include some additional information that will also help to clarify this section.
2012 IBC: “Electric locking systems, including electromechanical locking systems and electromagnetic locking
systems, shall be permitted to be locked in the means of egress in Group I-1 or I-2 occupancies where the clinical needs of persons receiving care require their containment.”
Many of the requirements of this section did not change, including the following means of unlocking the door:
- activation of the sprinkler system / fire detection system (a system is required in order to use these locks)
- loss of power to the locking system
- remote release from an approved location
- ability to be unlocked by clinical staff at all times (procedures must be part of approved emergency plan).
Building occupants must not be required to pass through more than one of these locked doors before entering an exit, and emergency lighting is required at the door. A new requirement for the 2015 edition is that the system must be listed per UL 294.
There are 2 exceptions now listed in this section – 1 for psychiatric treatment areas and 1 for nursery and obstetric areas of a Group I-2 hospital, where a listed egress control system is used to reduce the risk of child abduction. In both types of units, the doors are not required to unlock automatically; they are exempt from the requirements to unlock upon fire alarm, power failure, and remote release, and the limitation on the number of controlled egress doors before entering an exit does not apply.
The exception for child abduction systems clarifies that this section can be applied to units beyond memory care, which is the most common location for controlled egress locks. And exempting nursery and obstetrics units from automatic unlock would provide added security over a delayed egress lock, as well as removing the need for an audible alarm. With controlled egress locks, it’s less likely that the father in the video would have been able to remove the baby, but staff members must also understand security protocols as well as egress requirements.
Refer to the code sections from the IBC or NFPA 101 for additional information, and keep in mind that a particular edition of a code must be adopted in a facility’s jurisdiction before the requirements apply to that facility.
You need to login or register to bookmark/favorite this content.


This illustrates the unfortunate need for a secondary system.
Although infant abduction is rare, it almost always involves a family member (as in this case) or a mentally unstable middle aged woman (sad but true).
Infant protection, RFID tagging, although a costly addition helps staff recognize the situation.
Not that a tag can’t be removed.
Kudos to the CCTV installation great camera views surely helped law enforcement in preventing a most certain infant death.
Frank